Versão HTML básica



363
Clinical course and prognostic factors of children with Burkitt’s lymphoma in a developing country: the experience of a single centre in Brazil
Rev Bras Hematol Hemoter. 2012;34(5):361-6
phase of chemotherapy and two after recurrence of the tumor
in the CNS. The deaths were attributed to infection (n = 4),
tumor lysis syndrome, refractory disease (n = 3) and “malignant
hyperthermia” (n = 1). No information about the immediate
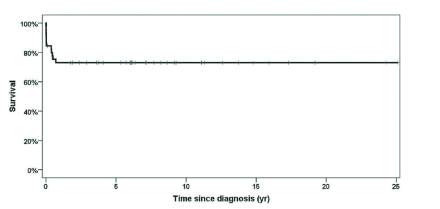
cause of death was available for three patients. The estimated
OS for all patients was 73% (Figure 1). The likelihood of OS for
patients with localized disease and advanced disease was 92.3%
and 67.7 %, respectively (p-value = 0.1 - Figure 2). Age, gender,
LDH, potassium, urea, creatinine and nutritional indices were
not significantly associated with patient outcome
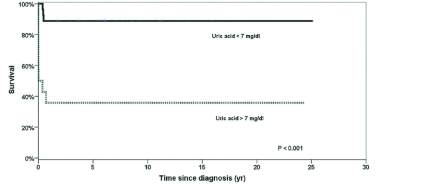
(Table 2). OS
was 89.2% for patients with uric acid of less than 7.0 mg/dL at
diagnosis and 35.7% for patients with uric acid levels of 7 mg/dL
or higher (p-value < 0.001 - Figure 3).
more than one site of involvement; two had the involvement of
abdomen and thorax and one had the involvement of the abdomen
and paravertebral region. Of the patients with abdominal tumors, 18
underwent laparotomy, with total resection of tumor in 12 (26.7%)
and partial resection in six (13.3%). Most patients had advanced
disease (31 patients - 68.9%). Stage was reported for 44 patients: 13
were Stage II (28.9%), 28 Stage III (62.2%) and three Stage IV
(6.7%). Serum LDH levels at diagnosis were available for 22 of
the 45 patients with mean serum LDH being 676.5 IU/L (range:
112 to 7407 IU/L). Serum uric acid levels were available for 42
patients with a mean value of 5.4 mg/dL (range: 0.8 to 41.0 mg/dL).
For 40 patients, the mean serum urea and creatinine levels were
23.5 mg/dL and 0.6 mg/dL, respectively. Serum potassium was
available for 29 patients, with a mean value of 4.2 mEq/L (range:
3.0 to 5.2 mEq/L). Eleven patients (24.4%) received the LSA2L2
protocol and 30 patients (66.7%) the BFM-83 protocol. The other
two patients were treated with other protocols and two patients died
before the start of chemotherapy.
Table 1 - Baseline clinical characteristics of 45 children with Burkitt’s
lymphoma (n = 45)
Characteristic
n (%)
Gender
Male
33 (73.3)
Female
12 (26.6)
Clinical presentation (site)
Abdomen
30 (66.7)
Mediastinum
3 (6.7)
Facial
6 (13.3)
Other sites
6 (13.3)
Clinical stage
I-II
14 (31.1)
III-IV
31 (68.9)
Diagnostic procedure
Cytopathology
5 (11.1)
Biopsy and histological examination
40 (88.9)
Immunophenotyping
29 (64.4)
Nutritional status (WAZ)*
< -1.28
15 (33.3)
> -1.28
30 (66.6)
Nutritional status (HAZ) †
< -1.28
8 (20)
> -1.28
32 (80)
Age at diagnosis (years) Mean (range)
4.7 (11.5 m – 13.2 y )
* WAZ: Z score for weight in relation to age
† HAZ: Z score for height in relation to age; there was no record of height at admission
for 5 children
Outcome
Complete remission was observed in 38 patients (84.4%).
During follow-up (median: 35 months; range: 1 to 60 months),
33 patients (73.3%) were alive at the first CR. Twelve children
(26.7%) died, two of them soon after admission without
receiving anticancer treatment. Eight died during the initial
Figure 1 - Survival of 45 patients with Burkitt’s lymphoma. Small vertical
lines on the curve represent patients alive at follow-up (Kaplan-Meier)
Figure 2 - Survival of 45 patients with Burkitt’s lymphoma, stratified by
localized
versus
advanced clinical stage. Small vertical lines on the curve
represent patients alive at follow-up (Kaplan-Meier; log-rank test for
comparison between survival curves)
Figure 3 - Survival of 45 patients with Burkitt’s lymphoma, stratified
by serum uric acid. Small vertical lines on the curve represent patients
alive at follow-up (Kaplan-Meier; log-rank test for comparison between
survival curves)